Thomas Edmunds Price is a Republican politician currently serving as the U.S. Representative for Georgia’s 6th congressional district (Atlanta suburbs) since 2005.
He is a physician who specializes in Orthopedic Surgery. He graduated medical school from the University of Michigan and completed his residency at Emory University.
Price has sponsored many bills over the years offering an alternative to the Affordable Care Act (Obamacare), which Republicans consider a quintessential piece of their list of programs to reform America called “A Better Way”.
Jun 2007: H.R. 2626 – Comprehensive HealthCARE Act of 2007
Jul 2009: H.R. 3400 – Empowering Patients First Act
Sept 2011: H.R. 3000 – Empowering Patients First Act (reintroduced)
Jun 2013: H.R. 2300 – Empowering Patients First Act of 2013 (reintroduced)
May 2015: H.R. 2300 – Empowering Patients First Act of 2015 (reintroduced)
June 2015: H.R. 2650 – Restoring Equity, Saving Coverage, and Undoing Errors Act of 2015
Feb 2016: H.R. 3762 – To provide for reconciliation pursuant to section 2002 of the concurrent resolution on the budget for fiscal year 2016. (Vetoed by President Obama)
After HHS released a report showing that health plans sold on the Health Insurance Marketplaces will increase by an average of 25% in 2017, Price released the following video on Oct 1st
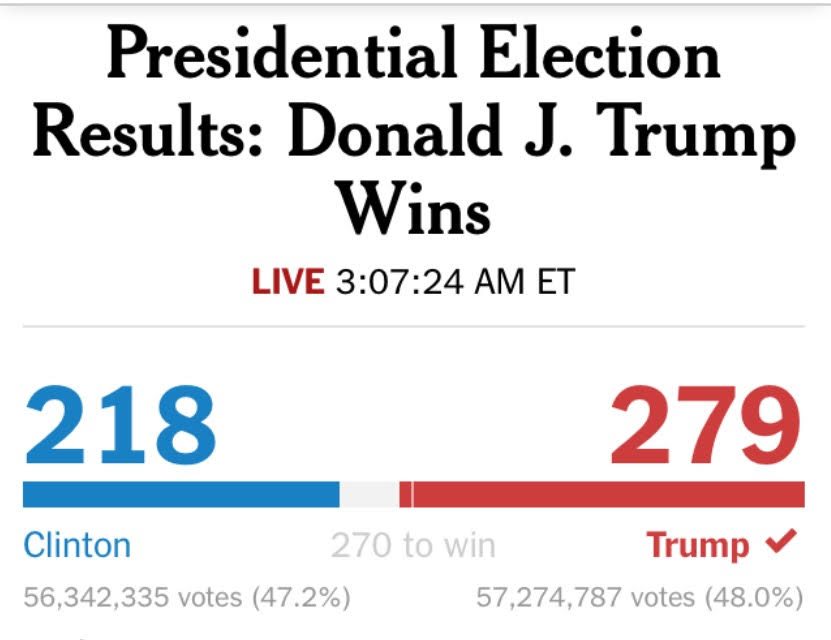
The last time one political party won the presidency three terms in a row was 27 years ago when George H.W. Bush won after Ronald Reagan’s two presidential terms from 1981 to 1989. Before that, 80 years ago Franklin D. Roosevelt served as President from 1933 to 1945 and passed the baton to another Democrat, President Harry S. Truman who served from 1945 to 1953. So it was always an uphill battle for Obama to continue his legacy through a Secretary Clinton presidential win.
Six Exit Polls from Last Night
Six exit polls from the New York Times help to explain yesterday’s election results. The polls collectively show “change” fatigue across the county. President Obama promised “change” and over the past 8 years successfully delivered upon that change. However, the overwhelming results of last night’s election shows that more than half of the country does not want to continue the country’s current track despite Obama’s favorable approval ratings.
Secretary Hillary Clinton was on the precipice of becoming the first female President of the United States. Despite the historic precedent of this achievement, she only won 54% of the female vote. She actually won less of the female vote than Barack Obama in 2012 who carried 55% of that vote. Despite the controversies surrounding Donald Trump with women, from alleged sexual improprieties to the leaked tape of his lewd comments, she was not able to marshal the female vote greater than 4 years prior.
If you felt the country was on the wrong track, you overwhelming voted for Trump. Tapping into the foreign trade deals that resulted in job losses throughout the Midwest flipped states like Wisconsin and Michigan.
If you felt the nation’s economy was either “Poor” or “Fair” you overwhelming voted for Trump as well. Unemployment ratings were reported being the lowest in over 5 years at 4.9% last month. However, while more Americans are working, their wages have declined. So despite the economy performing better over the past 8 years, the positive results were not felt by those Americans that voted for Trump.
The largest cohort in the county are White Americans without a four year college degree. A 2015 census report showed that roughly 113 million White Americans fall into this bucket. This cohort was most susceptible to the impacts of trade deals that moved jobs overseas and premium increases from the Affordable Care Act. This population overwhelming voted for Trump last night. Additionally, despite some controversial statements from Donald Trump regarding several minority groups including Muslims, Hispanics, and African Americans, roughly a fifth of non-white college graduates and non-whites without a college degree voted for Donald Trump as well. For comparisons, Obama won 51% of the population that did not have a college degree across all ethnicities.
George W. H. Bush, George W. Bush, and Jed Bush all publically stated the would not vote for Trump. Speaker Paul Ryan voted for Trump but publically told his fellow Congressman to run for re-election without endorsing Donald Trump. Many other famous Republicans aligned with the “Never Trump” movement looking desperately for another candidate. Nonetheless, Donald Trump still managed to capture 90% of the Republican vote; much higher than what the polls were showing. Donald Trump actually won his party’s votes 1% higher than Hillary Clinton who only won 89% of the Democrat vote. This was despite President Obama and Senator Bernie Sanders actively campaigning for her. Lastly, 48% of Independents voted for Trump; the exact opposite results of the 2012 and 2008 elections. While 15% of conservatives voted for Secretary Clinton, 10% of Liberals voted for Donald Trump.
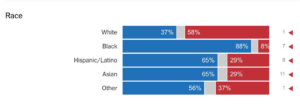
In 2012 Mitt Romney won 6% of the African American vote, 26% of the Asian vote, and 27% of the Hispanic/Latino vote. Donald Trump preformed better in 2016 across all categories. He won 2% more of the Black vote, 2% more of the Hispanic/Latino vote, and 3% more of the Asian vote despite his immigration policies and intentions to build a wall along the southern border.
4 Years Ago:Click Here to read what The Briefing Room wrote about the 2012 Election exactly 4 years ago.
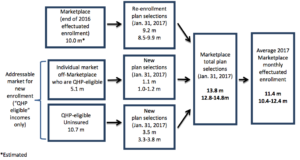
November 1st marks the start of the forth open enrollment period for President Obama’s Health Insurance Marketplaces. That means from today until January 31st, an estimated 10 million Americans who had coverage in 2016 will be able to renew their health plans online and an additionally 3.5 million Americans that still lack health insurance are expected to enroll into a health plan. However, not everyone is expected to enroll through the marketplaces. In fact, another 1.1 million Americans are expected to buy a health plan directly from a health insurance company, essentially bypassing President Obama’s Healthcare.gov enrollment website altogether.
However, even with all of this expected enrollment over the next three months, 11 million people that earn too much money for Medicaid will still remain without any health care coverage in 2017.
Source: U.S. Department of Health & Human Services, ASPE Issue Brief, “Health Insurance Marketplace Enrollment Projections for 2017” – October 19, 2016
How About The Headlines?
Headlines outlining the increase in monthly costs and available options for 2017 have bombarded the media since a report was released by the Department of Health and Human Services on October 24th. Just a few are listed below.
However, these headlines and articles only touch the surface of the true story. In fact, the widely reported price increases will actually only impact 3% of the entire U.S. population; roughly 10 million individuals.The vast majority of the country gets their insurance from their employer. Medical costs for most employer plans are expected to increase by only 6-8% in 2017.
Answers To Your Top Five…
1. What are the average increases in pricing for plans sold through the Health Insurance Marketplaces?
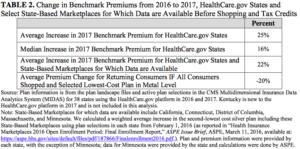
The average increase for States that use the HealthCare.gov website is 25%. The median increase is 16%. If you combine the States that use their own enrollment website (e.g.: New York & California), the overall average increase is 22%.
However, the increases in pricing is based on the “benchmark” plans. That is the way the website is able to determine financial assistance for Americans based on their income. Those benchmark plans are the second cheapest silver plans available to consumers to purchase. So, if every consumer selected the lowest-priced plan, consumers would actually see a -20% decrease year over year.
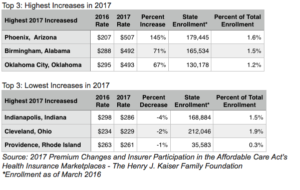
2. What are some examples of the highest and lowest pricing changes for 2017?
The year over year price changes below are what amounts expected by the health insurance company, regardless if it’s paid directly by the consumer or indirectly from the Federal Government. However, due to the financial assistance programs available to consumers based on their income, many Americans will not actually pay the full monthly prices listed below.
3. How does Financial Assistance help with the 2017 price increases?
Consumers who earn less than 4x the federal poverty level are available for financial assistance on a sliding scale. That means someone earning up to $47,520 per year or a family of four earning $97,200 per year in the 48 contiguous States & Washington D.C. are eligible for financial assistance. This helps to defray the monthly costs of buying healthcare coverage.
Example: John is a 27-year-old making $25,000 in Dallas, TX for 2017
$25,000 per year equates to 2.1x the federal poverty level. That means the maximum monthly costs for the second-lowest silver benchmark plan must be $142/month.
The actual monthly total cost of the second-lowest silver benchmark plan is $232/month.
That means financial assistance available to John is up to $90/month. ($232 – $142 = $90)
4. What does financial assistance mean for the rest of the country?
The marketplaces will continue to offer affordable coverage options:
More than 7 out of 10 will find a plan that is $75 or less a month.
Close to 8 out of 10 will find a plan that is less than $100 a month.
On average, consumers will have 30 health plans to choose from.
8 out of 10 consumers will choose from 2 or more health companies in 2017.
However, just because consumers can switch to cheaper plans does not guarantee they will find plans with low co-payments and deductibles. For example, many of the cheapest plans in the Health Insurance Marketplace have relatively high deductibles reaching $3,000 or more for an individual; doubled for families.
5. So, who will still lack health insurance coverage in 2017?
There are roughly 11 million people next year eligible to enroll in a health plan on the Health Insurance Marketplace but will remain uninsured in 2017.
8 out of 10 make between $11,880 and $47,000 per year as individual income earners.
6 out of 10 make between $11,880 and $29,000 per year as individual income earners.
A little more than half of them are males.
40% are aged between 18 – 34 years old; 40% are aged between 35 – 54 years old.
25% are Hispanic, 12% are African American, and 3% are Asian American.
31% are white males and 26% are white females.
71% have lacked health coverage for more than 1 year.
Source: ASPE Office of Health Policy – Health Plan Choice and Premiums in the 2017 Health Insurance Marketplace – October 24, 2016
In a recent trip to Thailand, I was amazed by the beauty and peacefulness of the country. When I first landed, the Thai people that greeted me in the airports and taxis quickly told me they were known as the Land of Smiles. However, it was not until I fully immersed myself into the daily city life of Chiang Mai, Bangkok, and Phuket, that I fully understood what they meant. Everyone I met was cordial and polite with a lightness about them. Many were Buddhists with a high regard for nature and the environment. It struck me how comfortable they were with the world around them. Since there is a strong belief in reincarnation, it seemed there was less of a burden living like you only have one chance to get it right. That spirit permeates throughout the country and allows for a carefree atmosphere wherever you go.
About Thailand
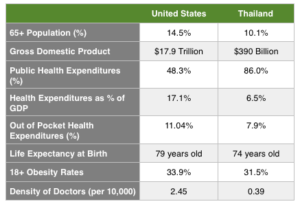
With over 67 million people and a $390 billion GDP (based on 2016 IMF estimates), Thailand ranks 28th out of 191 countries in economic wealth. Their healthcare system also ranks fairly high at 47th out of 191 countries based on the 2000 World Health Organization (WHO) report on healthcare systems. In comparison, the United States ranks #1 in GDP with a healthcare system ranked at #37. The WHO calculates healthcare rankings by analyzing how countries balance both the quality and equity of the healthcare services provided against the efficiency of its delivery.
For the past 14 years, Thailand has been able to do what the United States has not, despite the passing of the Affordable Care Act. Since 2002, Thailand has offered affordable, high quality healthcare universally across the entire country.
Offering universal healthcare coverage was no small task. The Thai people are very diverse. Among the largest minorities living in the country are ethnic Lao (25%), ethnic Khon Muang (10%) and many others from the neighboring countries of Burmese, Cambodians, and India. The population is growing as well; 0.3% annually with net migration of 100,000 people per year. To make things harder, a little more than half of the country lives in urban areas leaving the other half in much harder to reach rural and mountainous areas. Developed nations that have been able to provide universal healthcare usually have homogenous populations, which make it much easier to deliver healthcare services to the entire population.
So How Did They Do It?
It starts with a country’s constitution. If it is not part of the moral fabric of the country, universal healthcare will never become a reality.
The right of every Thai citizen to access health care and the right of the poor to free health care were addressed in the 1997 and 2007 constitutions, and access to health services for all was part of the 8th National Social and Economic Development Plan (1997-2001). – Thailand’s Universal Coverage Scheme: Achievements and Challenges.
Thailand achieved universal health care in 2002 after decades of trial and error. Prior to the change, more than 30% of the country lacked coverage. The Universal Coverage Scheme (UCS) was credited with covering 75% of the country. This included 18 million people previously uninsured. The remaining 25% received their coverage as either a government employee or private-sector employee. In comparison, close to half of the United States receives healthcare coverage from their employer; a much higher percentage than Thailand. Additionally, only 15% of the U.S. was uninsured before the Affordable Care Act passed; roughly 45 million people. However, after 3 years of the law in the U.S., only 20 million people have received coverage. That means Thailand was able to enroll as many people in one year it has taken the United States to enroll in 4 years of Healthcare reform.
In the 10 years since the UCS was enacted, the Thai healthcare system continues to be successful. Lower income people have greater access to care. This has been seen with increased outpatient and hospital visits by the poor. Additionally, the rate of those who became poor due to healthcare expenses declined radically from 2.71% in 2000 to 0.49% in 2009. Lastly, customer and physician satisfaction rates are up to 90% and 79% respectively.
Financing Universal Healthcare
Federal funds finance the UCS at a high enough level to ensure healthcare services are free of charge to those that need it the most. The benefits offered under the plan focus on preventive care, health promotion, and disease prevention. There is also a fixed budget with caps on physician payments, which help to control costs. The biggest change in the reform was the focus on primary care. Specifically, the UCS ensures that the Thai people visit their primary care physician who then coordinates their health care through the healthcare continuum. Additionally, Thailand already had a strong healthcare infrastructure as a foundation. Physicians receive capitation and case-based payments with a global health budget. That is, they received a fixed amount of money at a local level to take care of the healthcare needs of the population they serve within their district.
Under this new healthcare model, the “near poor” who struggled the most now have a pathway to affordable care. Out of pocket health care costs used to account for 33% of total costs. This has now declined to less than 8%.
Roughly 47 million people receive their coverage through the UCS. With more people accessing coverage, healthcare costs grew by more than 71% from 2002 to 2011. That was an increase from 1,202 baht to 2,693 baht per capita. Increased costs were mostly driven by higher labor costs for healthcare physicians and increases in utilization; people using more services every year. However, despite these increases, the Thai government works collectively to ensure the UCS remains sustainable. The constitution serves as their mission, vision, and guiding principles.
A person shall enjoy an equal right to receive standard public health services, and the indigent shall have the right to receive free medical treatment from State infirmaries. The public health service by the State shall be provided thoroughly and efficiently. The State shall promptly prevent and eradicate harmful contagious diseases for the public without charge. – The 2007 Thai Constitution
Lessons from the Land of Smiles
1. Adopt universal healthcare policies that cover a large percentage of the population. This will encourage the program’s success and sustainability. Over 75% of the country receives their healthcare coverage from the Universal Coverage Scheme compared to American where less than 10% receive their coverage from the Affordable Care Act’s Health Insurance Marketplaces.
2. Invest in the poor across all areas of their lives, not just healthcare. Thailand has learned that helping the poor will consequently improve the economics of the entire nation. They have consistently invested in the social fabric of their country seen by their high literacy rates, very low unemployment rates, and the lowest food deficit rates in the region. All these factors assist with eliminating the barriers caused by socioeconomic factors.
3. Focus on health promotion and healthcare prevention. Thailand has been able to emphasize the role of primary health care and the rational use of effective and efficient integrated services. Thailand also ensures proper referrals to high quality hospitals. Lastly, the county has eliminated any of the out of pocket expenses for preventive care.
Sources: World Health Organization Global Health Expenditure database
Thailand’s Universal Coverage Scheme: Achievements and Challenges. An independent assessment of the first 10 years (2001-2010). — Nonthaburi, Thailand: Health Insurance System Research Office, 2012. 120 p.
“It was the best of times, it was the worst of times. It was the age of wisdom, it was the age of foolishness, it was the epoch of belief, it was the epoch of incredulity, it was the season of Light, it was the season of Darkness, it was the spring of hope, it was the winter of despair, we had everything before us, we had nothing before us, we were all going direct to heaven, we were all going direct the other way” – Charles Dickens, A Tale of Two Cities
The words of Charles Dickens can perfectly describe our current Presidential election as well as the state of Healthcare reform in this country. Last night’s second Presidential debate finally broached the subject of healthcare. Twenty-four minutes into the debate, the candidates received their first healthcare question. Secretary Clinton and Mr. Trump were able to discuss the merits of their healthcare policies for the next 7 minutes and forty-five seconds.
“Affordable Care Act, known as Obamacare, it is not affordable. Premiums have gone up, deductibles have gone up, copays have gone up, prescriptions have gone up, and the coverage has gone down. What will you do to bring the cost down and make coverage better?” – Question from the audience.
Clinton
Secretary Clinton agreed with many of the sentiments expressed in the question but reminded America about all the positive aspects of the law. She explained when the law passed in 2010, it was not just focused on the 45 million Americans that lacked insurance at the time, but also improved the coverage of the roughly 170 million Americans that already received healthcare coverage from their employer.
She outlined the following key provisions of the Affordable Care Act that helped those Americans already insured:
Elimination of lifetime limits: Health plans can no longer stop covering a consumer when their health costs reach a certain dollar amount.
Elimination of Pre-existing conditions: Health plans can no longer deny coverage to consumers who enroll already diagnosed with a sickness or disease.
Expanded Coverage up to Age 26: Health plans now cover children up to age 26 regardless of educational status. This was expanded from the old limits of age 19 or up to 23 for fulltime students.
Many of these provisions extended coverage to those Americans who cost more to the Healthcare system. As such, these features indirectly correlated to the premium, deductible, and copay increases Americans have faced since 2014. Many healthcare policy experts warned us of this issue asserting that the Affordable Care Act would increase costs early on as more people got expanded benefits. Healthcare costs would only begin to stabilize and decline over time.
Lastly, the Department of Health & Humans Services released a report on September 29th outlining the “historic, widespread increase in Health insurance coverage”. Specifically, 20 million Americans have gained health coverage as a result of the Affordable Care Act. That is close to a 50% decrease in the amount of people that lacked health coverage in 2014; the 1st year of the Health Insurance Marketplaces. In 2010 , 16% of the country lacked coverage, it has lowered to 8.6% through March 2016. The gains in health coverage were seen across all demographics including race, income, age, and geography.
Secretary Clinton is leery on repealing the entire law and starting from scratch. She wishes defend and extend the law: continue the provisions that work and improve the ones that do not. However, she did not provide specifics on how she would get that done.
“Right now we [have] 90% Health insurance coverage. That’s the highest we’ve ever been in our country. So I want us to get to 100% but get costs down and keep quality up.” – Secretary Hillary Clinton
Trump
Donald Trump started his comments laser focused on the premium increases certain Americans will be facing in 2017. The McKinsey Center for U.S. Healthcare Reform reports that next year will be the highest increase of monthly prices for health care coverage through the Health Insurance Marketplaces since its inception. In 2014, the median increase ranged from 2.7% for Bronze plans to 6.6% for Platinum plans. In 2017, the median price increases will range from 7.6% for Platinum plans up to 17.1% for Catastrophic plans. Ironically, Catastrophic plans were specifically designed to attract young and healthy people. Those plans have the highest deductibles and are specifically sold Americans under the age of 30 that lack insurance coverage due to the costs.
Without using specifics, Donald Trump alluded to states like Tennessee that will see 25% rate increases for their Health Insurance Marketplace plans in 2017. This is the second year in a row consumers in Tennessee will see increases over 20%. Even large national health care plans will average 27% rate increases in 2017. Competition appears to be dwindling as well. Many health plans have started to exit certain states.
2017 Health Insurance Marketplaces – Average Health Plan Rate Increase
42% will receive single digit increases up to 10%
30% will receive double digit premium increases over 10%
20% will receive premium decreases of 10% or less
Only 8% will receive premium decreases more than 10%
Donald Trump also focused on costs, properly mentioning that healthcare is one of the most expensive line items in the Federal budget. He believes costs are on the rise because of the lack of competition. His remedy is to increase competition by eliminating the current barriers health companies face selling coverage over state lines.
However, he failed to mention that medical cost trends have declined from a 11.9% annual increase to a projected 6.5% in 2017. That would be the lowest cost trend increase we have seen in years. The declines have been seen in physician costs, which have been offset by increases in prescription drug costs and utilization.
While Trump strongly calls for the repeal and replacement of the Affordable Care Act, he failed to provide any details or specifics on his alternative approach. He also did not specify which portions of the Affordable Care Act would also be in his replacement plan. It is hard to ascertain whether Trump is for or against mandated coverage for all Americans, health insurance market places, the elimination of pre-existing conditions, or the elimination of lifetime limits. He did however hint at agreeing with Paul Ryan’s budget plan which calls for block grants to states to administer the Medicaid program. Health policy analysts and Democrat Governors are leery on this idea since it would inevitably lead to spending cuts to Medicaid. Since 2014, Medicaid growth has been exponential.
“Not only are your rates going up by numbers that nobody believes, but your deductibles are going up. So that unless you get hit by a truck, you’re not going to be able to use it. It is a disastrous plan and it has to be repealed and replaced.” – Donald Trump
Healthcare was barely mentioned during the ninety-minute Presidential debate between Secretary Hillary Clinton and Real Estate mogul, Donald Trump back on September 26th.
Both campaigns have a chance to redeem themselves with tonight’s first and only Vice Presidential debate that will be held tonight at Longwood University in Farmville, Virginia.
Mike Pence is the Republican Party nominee for Vice President and currently serves as the Governor of Indiana. He has a long history in politics, previously serving in the U.S. Congress since 2000. He rose to the position of chairman of the House Republican Conference in 2011 before leaving Congress to run for Governor.
Tim Kaine is the Democrat Party nominee for Vice President. He currently serves as a U.S. Senator representing Virginia. He chaired the Democratic National Committee for four years and served as the Governor of Virginia. He too held past roles in government as the Lieutenant Governor of Virginia and the Mayor of Richmond.
On To The Debate
Similar to the Presidential debate, it will last for 90 minutes without commercial breaks. Elaine Quijano, CBS News anchor and correspondent, will serve as the moderator. She will personally make history serving as the first Asian American moderator for a general election debate.
The debate will be divided into nine 10 minute segments. After an opening question, the Vice Presidential candidates will have 2 minutes to respond. The remaining time will be used to further discuss the issue at hand.
There is an even greater burden on Ms. Quijano tonight, since Lester Holt did not bring up healthcare in the prior debate. Even though the Vice Presidential candidates historically serve as surrogates to the candidate at the top of the ticket, both VP nominees have a storied history on Healthcare themselves that should be examined tonight.
MIKE PENCE ON HEALTHCARE
Governor Pence took the Indiana Governorship in 2013. At that time over 15% of Hoosiers lacked health insurance coverage. As of today, the uninsured rate has dropped to 9.6%. Despite this success, Mike Pence voted against the Affordable Care Act in 2010 as a congressman. In fact, when the law passed Politico reported that compared it to the September 11th terrorist attacks.
Pence later co-sponsored HR 6079 in 2012, which was one of many bills seeking to repeal the Affordable Care Act. Ironically, the fiscally conservative Congressman co-sponsored and voted for a bill that the CBO stated would add $109 billion to federal budget deficits from 2013 to 2022.
While repealing the law would generate $1.1 trillion in savings; the CBO said it would also cause an increase in direct spending of $711 billion and reduced tax revenues of $569 billion which equated to more than the savings generated by the repeal.
Oddly enough though, Mike Pence as Governor implemented the expansion of Medicaid, a key feature of the Affordable Care Act, despite fighting to repeal the law as a congressman serving the same state.
It should be mentioned that Pence’s implementation of the Medicaid expansion was one of the most complex of the entire nation. He did, however, implement the expansion leveraging many Republican/Conservative principles.
Hoosiers now have:
Access to “Personal Wellness & Responsibility” health savings accounts, a key feature of many Republican health care reform bills.
To pay monthly premiums for Medicaid coverage depending on their income and health status.
Can purchase a more enhanced Hoosier Insurance Plan (HIP) with access to more benefits if they pay the monthly premium. This is a key Republican provision that seeks to ensure even low income Americans have accountability and skin in the game for their healthcare coverage.
Can only receive non-emergency medical transportation after 1 year once it is deemed medically necessary.
Some provisions were even denied by CMS such as requiring Medicaid members to show they were employed to continue enrollment in the health plans.
Lastly, in 2016, four companies announced they would be exiting the market in Indiana by the end of 2016: UnitedHealthcare, Southeastern Indiana Health Organization, Physicians Health Plan, and Indiana University Health Plans. This was mainly due to the financial losses these companies felt 3 years into the Affordable Care Act’s Health Exchanges. There are a little under 200,000 Hoosiers that will negatively be impacted by these market changes.
Pence is pro-life similar to Tim Kaine. However, unlike Kaine, he has aggressively voted to defund Planned Parenthood. He also voted on many anti-abortion bills that some have called extreme. Most recently, Pence signed an aggressive anti-abortion bill into law in March of this year that creates many hurdles for mothers to access the service.
Questions to ask him tonight:
Question 1: As a fiscally conservative Republican, please explain the co-sponsorship of a bill to repeal the Affordable Care Act that would raise the federal deficit by $109M?
Question 2: As a congressman, you voted multiple times against the Affordable Care Act, yet as Governor you expanded Medicaid in your state. How do you rationalize being for the Affordable Care Act after you were against it? What changed between the halls of Congress and Governor’s mansion. Please be specific.
Question 3: Indiana lags the nation in lowering the uninsured rates, so why should we believe a Trump/Pence administration would be better for America? Please offer up to three specifics.
TIM KAINE ON HEALTHCARE
Tim Kaine was Governor of Virginia from 2006 to 2010. The uninsured rate in Virginia was 14.1% when Kaine entered office. By 2010, it increased 0.5% to 14.6% leaving more than 1 million Virginians without health insurance coverage. The vast majority of those uninsured were aged 19-64, earned 200% of the federal poverty level or below, and had at least one person working in the family. Interestingly enough, Virginia residents who were not US citizens were three times more likely to be uninsured during his Governorship. Secretary Clinton has discussed at lengths expanding the Affordable Care Act to those who are undocumented and in the United States.
While Kaine was not in Congress to vote on the Affordable Care Act, he has been a vocal proponent of the law as the head of the Democratic National Committee. He even co-sponsored S.2782 (States Achieve Medicaid Expansion Act) in 2016 which sought to provide financial incentives to states reluctant to expand Medicaid. CBO estimates as of 10/3 have not been received on this bill to see how it would impact the deficit.
The Affordable Care Act has yet to insure all Americans. There are still roughly 30 million Americans that lack insurance. Additionally, health insurance premiums have skyrocketed since the implementation. Virginia has seen rate increases as high as 28%. In 2016 alone, Virginia witnessed UnitedHealthcare threaten to leave the state and Humana officially exit the state. These changes greatly impact the 378,000 Virginians currently getting health care coverage through the Affordable Care Act.
Kaine is also a Senator of a state that is reluctant to expand Medicaid despite their Democrat Governor, Terry McAuliffe being a proponent of the law. If Virginia expanded Medicaid it would help cover 131,000 people who earn too much for Medicaid, but not enough income to get financial assistance through the Affordable Care Act. Additionally, another 462,000 would be eligible for Medicaid benefits under the increased income guidelines.
Kaine is known as personally pro-life, however backs many pro-choice legislations including Planned Parenthood. Under his term, Virginia was the first state to require all girls to get the HPV vaccine. Lastly, and maybe most notably, as Governor, Kaine signed a $42 million package to overhaul mental health services after the 2007 mass shooting at Virginia Tech.
Questions to ask him tonight:
Question 1: The uninsured rate in your state increased under your Governorship. Please explain why the American people should trust you in your pursuit to “defend and further extend” the Affordable Care Act? Please offer up to three specific reasons.
Question 2: Americans continue to see double digit increases on their health insurance premiums and health plans continue to exit the market year after year. In fact, your home state of Virginia has not expanded Medicaid under the Affordable Care Act provisions. Why do you believe the law is working for America? Please offer up to three specific reasons.
Question 3: The Affordable Care Act as written does not offer insurance coverage to undocumented Americans; however they are the most uninsured individuals in your state. Your platform seeks to expand access to healthcare regardless of someone’s immigration status. How do you intend to implement and pay for this for Virginia and the rest of the nation?
Tonight, we will witness the much anticipated Presidential debate being held at Hofstra University in Hempstead, New York, between two longstanding New York powerhouses: Secretary Hillary Clinton and Real Estate mogul, Donald Trump. We should hope there is time for the candidates to clearly outline their healthcare policies and proposals.
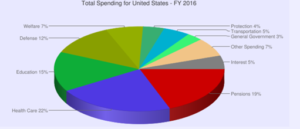
Why Healthcare?
Healthcare will represent over 22% of total Federal, State, and Local Government spending in 2016. Expenditures are projected to be close to 20% of GDP as well. However, despite representing 1/5th of the economy and government spending, Presidential debates have not historically spent the same proportional time on the topic.
Healthcare has always been viewed as third rail in politics. The big two programs that make up most of the Healthcare spending are Social Security and Medicare. Even the staunchest laissez-faire capitalist have steered clear of proposing spending reforms on such popular programs despite their looming insolvency. The 272 paged 2016 Annual Report from the Social Security and Medicare Board of Trustees projects shortfalls in Social Security to begin in 2034; just 18 years away. Likewise, Medicare is projected to have depleted funds by 2028; at which time the funds will be sufficient to pay only 87% of Medicare Hospital Insurance costs.
New York, NY
Coincidentally, New York serves as a relevant backdrop for the 1st presidential debate of this year’s campaign; especially when it comes to Healthcare. New York serves as an interesting microcosm for all the threats and opportunities the nation is facing with runaway healthcare costs. Since the Affordable Care Act has passed, New York has had as much good news as bad news.
The Good News: Since the law passed, the number of New Yorkers without insurance decreased by 850,000. The uninsured rate has been cut in half from 10% to 5%; the lowest rate in decades. Many of those that gained coverage enrolled in Medicaid, which has helped hospitals lower the rate of healthcare services delivered to people who lack the means to pay for it (uncompensated care).
The Bad News: Health Republic, the largest Health Exchange/Affordable Care Act healthcare plan in 2014 went out of business in less than two years. Many other large health insurance companies had also pulled out of the market stating unsustainable market conditions. NY hospitals continue to struggle financially stimulating downsizing, closures and mergers. Since 2000, 19 hospitals have closed in just New York City.
On To The Debate
Lester Holt has a very important task as tonight’s debate moderator. It is imperative that the candidates highlight their policy positions. That requires the right environment for a true policy discussion to take place.
The debate will be ninety minutes long split up into six different fifteen minute segments. Healthcare should be one of those segments. The moderator will open each section with a question and candidates will give alternating two-minute responses followed up with 10 minutes of open discussion. There will be no commercial breaks and crowd feedback will be limited.
DONALD TRUMP ON HEALTHCARE
Click Here for Donald Trump positions on Healthcare
Questions to ask him tonight:
Question 1: What will be the top three impact to the millions of americans currently receiving health insurance coverage through the Affordable Care Act after it is repealed and replaced by your administration? Please be specific.
Question 2: Based on your policy to end the “individual mandate”, how will you incentivize young healthy people to enroll into healthcare plans so that the insurance pools stay balanced and stable?
Question 3: Many worry that the removal of the barriers that inhibit the sale of health insurance across state lines would create a race to the bottom; meaning the states with the most relaxed rules and provisions would end up insuring a disproportionate share of the country. Is there anything in your policy position that will prevent that from happening?
HILLARY CLINTON ON HEALTHCARE
Click Here for Hillary Clinton positions on Healthcare
Questions to ask her tonight:
Question 1: In your pursuit to “defend and further extend” the Affordable Care Act, please offer up to three specific ways you will bring down the high out-of-pocket costs of deductibles and copayments while simultaneously keeping health plans affordable? Usually lower deductibles mean higher monthly premiums.
Question 2: In our free market economy, please give up to three specific ways on how you plan to reduce prescription drug spending by protecting consumers from unjustified price increases on life saving drugs?
Question 3: The Affordable Care Act as written does not offer insurance coverage to undocumented Americans; however your platform seeks to expand access to healthcare regardless of someone’s immigration status. Please discuss how this would work and specifically how this program would be paid?
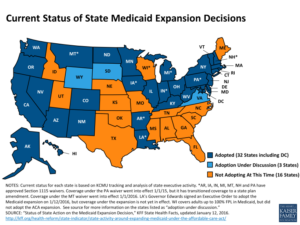
Out of the six remaining major Republican candidates for President, only two remain that can claim “Executive Experience”; former Governor Jeb Bush of Florida and Governor John Kasich of Ohio. On Saturday, February 13th the two Governors squared off during the Republican debate, tackling questions around expanding Medicaid programs while maintaining conservative values.
Jeb’s Replacement Plan
Jeb Bush has actively campaigned to repeal and replace the Affordable Care Act (Obamacare). However, there has been little discussion publically about what the replacement would look like. He also has publicly challenged John Kasich on his conservative record because Ohio actually used the Affordable Care Act to expand Medicaid to Ohioans that were making up to roughly $16,000/year. Jeb was instrumental in ensuring that Florida did not make that same decision. In fact, Florida joined 18 other states that have not expanded Medicaid since 2014. It was widely reported that Jeb met with Florida lawmakers back in 2013 and challenged them to come up with conservative alternatives to expanding Medicaid under the Affordable Care Act. One such alternative was a pilot program launched in 2005 that he dubbed “Empowered Care”. The program gave money to Medicaid recipients to buy their own healthcare plan from Health Insurance companies; while costs decreased, Florida still remained one of the states with the highest uninsured rates and in 2004, 25% of the uninsured were very poor. In fact, close to 50% of Florida’s uninsured workers earned less than $15,000 per year; the income level Obama’s Affordable Care Act was raised to Medicaid eligibility. So costs decreased, but less people had coverage. Kasich argues this is not conservative because uninsured Americans still need healthcare so the country ends up paying for them in more expensive places.
Kasich’s Conservative Justification
Kasich decided to expand Medicaid under the Affordable Care Act in Ohio, along with 31 other states. Ohio now has 2.9M people enrolled in a Medicaid or Child Health Insurance Program, which is an increase of 623,626 since September of 2013. More importantly 90.2% of all eligible children now have health coverage. More enrollment means higher costs overall. However, uninsured rates fell from close to 14% to 10.5%. How does the Medicaid expansion work, anyways? The federal government partners with each state to offer the Medicaid program. In Ohio, the Federal government pays for roughly 63% of the costs and the Ohio state government covers the rest. However, when Kasich decided to expand Medicaid and more people with higher incomes could join the program, the Federal government took on 100% of the costs of the newly enrolled people. This will soon shrink to 90% in 2020, but it will still be a higher percentage than the 63% they pay now for Ohioans that were enrolled in Medicaid before the expansion. An Urban Institute study showed that with the Affordable Care Act and Medicaid Expansion, Ohio’s uninsured would shrink from 1.6M people to only 635k people by 2022. Another net effect is employers pay less for employee healthcare since they can opt for Medicaid benefits. The forecasted savings is close to $1.7 billion for Ohio employers. More importantly is the savings projected for the Ohio consumer. Kasich discussed the savings that happen when uninsured and underinsured people seek care through Medicaid and not through the emergency room without coverage. When people have insurance and seek care pro-actively as opposed to episodical, overall costs. Estimates of potential savings were as high as $7.4 billion by 2022.
Kasich openly talks about how his state was facing a budget shortfall and now has a budget surplus of $2 billion. This would not have been possible without the confluence of many different state actions, including the expansion of Medicaid. Sometimes when Republicans defend Gov’t spending, it can be for conservative reasons.
Open Enrollment for the Health Insurance Marketplace will end on January 31st. That means there are only 7 more days to choose a health plan and enroll if you:
Make too much money for Medicaid (approximately $16,000/yr).
Are 64 years old or younger and cannot enroll in Medicare.
Are not getting health insurance coverage from your employer
Don’t feel bad if you’ve been procrastinating. Last year nearly 20% of all enrollees chose a health plan in the last month of enrollment.
So far, 2016 enrollment reached more than 11 million individuals as of the end December. If trends continue, that could mean 13.2 million people enrolling into a health plan by the end of January.
The Importance of Shopping
A new report released on January 21st from the Department of Health and Human Service uncovered the importance of shopping for a new plan. When consumers shopped, for the most part, they saved money.
43% of consumers actively chose a health plan in 2016. 60% of them switched plans.
After switching plans, consumers lowered their average monthly cost for healthcare from $179 to $137.
On average, consumers that switched plans saved 24% or $43 per month after financial assistant.
Financial assistance reduced the monthly premium for consumers by an average of 72%.
Availability of Health Plans below $100/month^
$50 or Less*
$75 or Less*
$100 or Less*
Plan Availability
59%
66%
72%
Actual Consumer Behavior
27%
39%
48%
^Enrollment figures from Healthcare.gov
*With Financial Assistance
As you can see, consumers did not avail themselves to all of the savings that were possible on Healthcare.gov. In fact, 28% of 2015 consumers were “auto-enrolled” into a new plan in 2016. When consumers did not actively shop for a new health plan, they were more likely to pay higher monthly costs for health coverage.
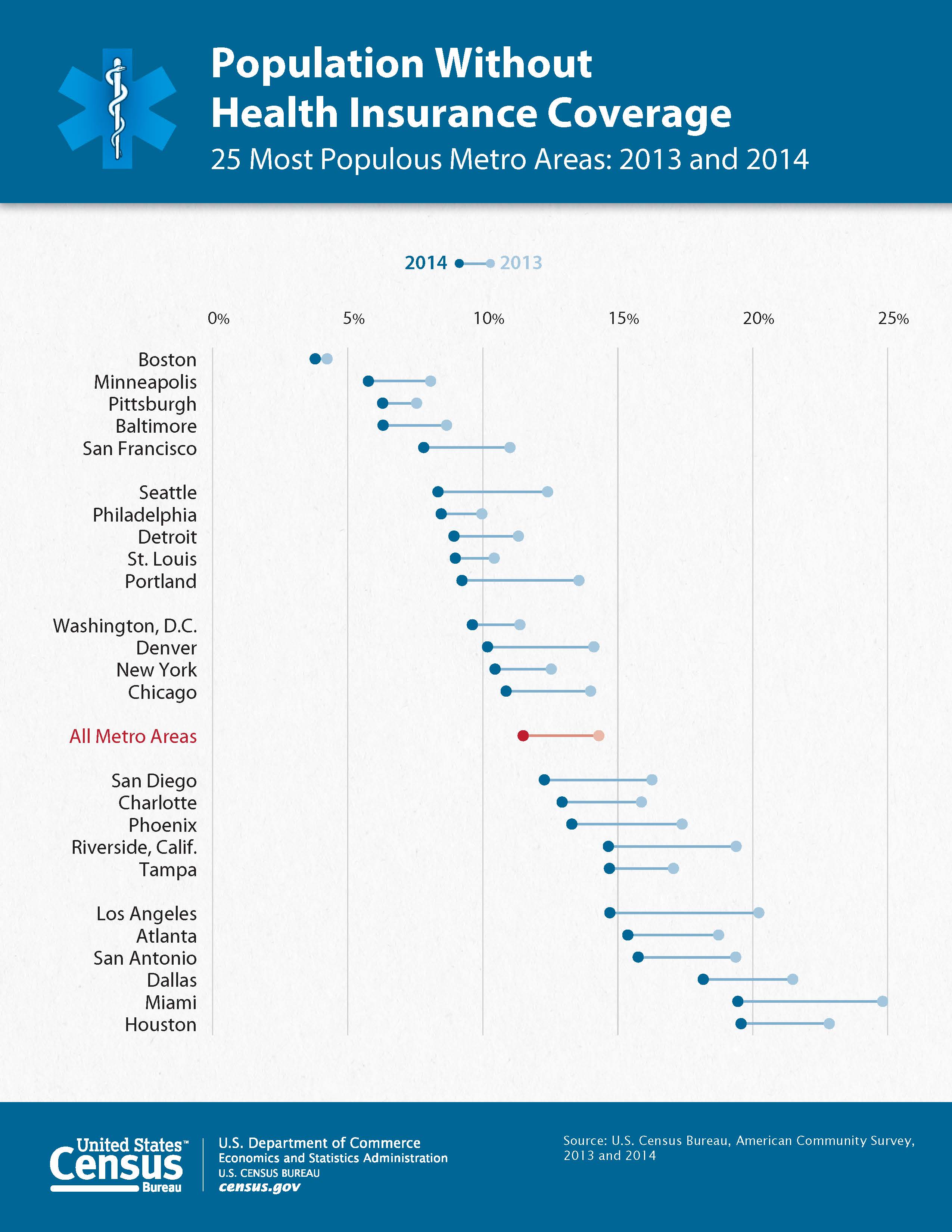
Highest Areas of Uninsured?
The following cities across America have the highest rates of people lacking health insurance that cannot enroll in a public program like Medicare or Medicaid.
Texas cities with close to 9% of the population lacking health coverage:
Harlingen, Texas
Weslaco, Texas
Burnsville, Texas
Boise, Idaho – 8% of the population lacks health coverage:
Tulsa, Oklahoma – 7.5% of the population lacks health coverage
Florida cities with +7% of the population lacking health coverage:
Fort Myers, Florida
Naples, Florida
Miami, Florida
Fort Lauderdale, Florida
Orlando, Florida
Daytona Beach Florida
Melbourne, Florida
Tampa, Florida
St. Petersburg, Florida
New Orleans, Louisiana – 7% of the population lacks health coverage
January 2016 marks the 3rd year of the Health Insurance Marketplaces, a key provision of the Affordable Care Act designed to help millions of Americans buy affordable, quality healthcare. In those three years, enrollment has grown to well over 12 million people. Thus far, 3 million new Americans enrolled in 2016. 35% of those enrolled are 35 years old or younger; an important statistic for the viability of the law. Without enough young enrollees with minimal healthcare usage, the prices for health plans could potentially skyrocket. 85% of those enrolled are receiving financial assistance, which make the costs of their health plans cheaper each month.
Overall, there was enrollment growth nationwide in 2016. However one city in particular had surprising figures and now ranks #1 in Obamacare enrollments. It’s a city named Hialeah located in South Florida.
Obamacare’s Favorite City
More than 66,000 residents from multiple zip codes in the City of Hialeah purchased health coverage on Obama’s Health Insurance Marketplace in 2016. That represents almost 1/3rd of Hialeah’s 225,000 residents. Open enrollment does not officially end until January 31st, which means the numbers can only improve. Zip code 33012 registered 14,760 enrollments alone representing the zip code with the highest Obamacare enrollment nationwide. Located in Miami-Dade County, Hialeah is a major city of the South Florida metropolitan area and is the 6th largest city in Florida.
92% speaking a language other than English in the home.
81% of the businesses are Hispanic-owned firms
The median household income is a little under $30,000 and close to 18% of Hialeah lives below the poverty line.
Close to 25% of the residents of Hialeah lacked health insurance.
Close to 18% of Hialeah lives below the poverty line with a median income; severely below the national average. Only 10% of their population has a college degree. And according to the U.S. Census Bureau’s American Community Survey – the City of Hialeah is in a county ranking one of the highest in the country has lacking health insurance –with 25%.
Hialeah Politics
Running on a less than popular Affordable Care Act, Barack Obama won the state of Florida for the second time (50.0% to 49.1%) against his Republican Presidential rival, Mitt Romney in 2012. Even more convincingly, President Obama also won Miami-Dade county 61.6% to 37.9% against Romney.
However, Hialeah had totally different results. Hialeah has one of the largest Cuban populations in the nation; a group that tends to overwhelmingly vote Republican. Additionally, Hialeah’s political leaders publically endorsed Mitt Romney in 2012 who ran to undo Obama’s health law. The list of endorsers included: Carlos Hernandez – Mayor of Hialeah, Yioset de la Cruz – Mayor of Hialeah Gardens, and various high profile Hialeah City councilmen and councilwomen. Lastly, a study by The Bay Area Center for Voting Research found that the City of Hialeah was the 4th most conservative city in America. 71% of the city’s registered voters select conservative candidates.
In the End
The City of Hialeah can be emblematic of the many cities across America that have benefited from policies that the residents strongly oppose; essentially voting against their personal and political interests. This could be an opportunities for party leaders to improve their political messaging and communication. In fact, the latest results from the Kaiser Health Tracking Poll shows 46% of American adults still have an unfavorable view of President Obama’s Affordable Care Act; an increase of 6% since April 2010.









 In a recent trip to Thailand, I was amazed by the beauty and peacefulness of the country. When I first landed, the Thai people that greeted me in the airports and taxis quickly told me they were known as the Land of Smiles. However, it was not until I fully immersed myself into the daily city life of Chiang Mai, Bangkok, and Phuket, that I fully understood what they meant. Everyone I met was cordial and polite with a lightness about them. Many were Buddhists with a high regard for nature and the environment. It struck me how comfortable they were with the world around them. Since there is a strong belief in reincarnation, it seemed there was less of a burden living like you only have one chance to get it right. That spirit permeates throughout the country and allows for a carefree atmosphere wherever you go.
In a recent trip to Thailand, I was amazed by the beauty and peacefulness of the country. When I first landed, the Thai people that greeted me in the airports and taxis quickly told me they were known as the Land of Smiles. However, it was not until I fully immersed myself into the daily city life of Chiang Mai, Bangkok, and Phuket, that I fully understood what they meant. Everyone I met was cordial and polite with a lightness about them. Many were Buddhists with a high regard for nature and the environment. It struck me how comfortable they were with the world around them. Since there is a strong belief in reincarnation, it seemed there was less of a burden living like you only have one chance to get it right. That spirit permeates throughout the country and allows for a carefree atmosphere wherever you go.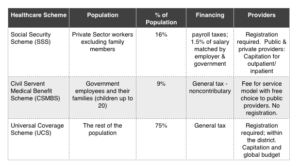
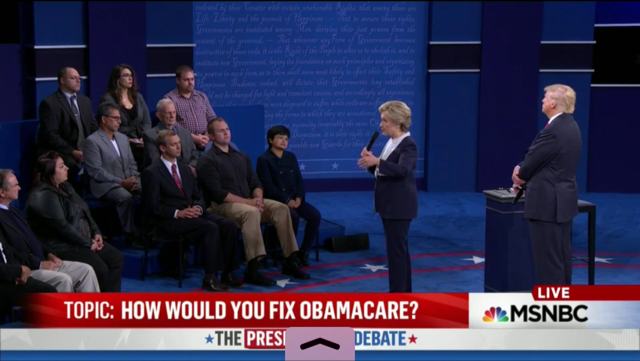
 “Affordable Care Act, known as Obamacare, it is not affordable. Premiums have gone up, deductibles have gone up, copays have gone up, prescriptions have gone up, and the coverage has gone down. What will you do to bring the cost down and make coverage better?” – Question from the audience.
“Affordable Care Act, known as Obamacare, it is not affordable. Premiums have gone up, deductibles have gone up, copays have gone up, prescriptions have gone up, and the coverage has gone down. What will you do to bring the cost down and make coverage better?” – Question from the audience. “Right now we [have] 90% Health insurance coverage. That’s the highest we’ve ever been in our country. So I want us to get to 100% but get costs down and keep quality up.” – Secretary Hillary Clinton
“Right now we [have] 90% Health insurance coverage. That’s the highest we’ve ever been in our country. So I want us to get to 100% but get costs down and keep quality up.” – Secretary Hillary Clinton “Not only are your rates going up by numbers that nobody believes, but your deductibles are going up. So that unless you get hit by a truck, you’re not going to be able to use it. It is a disastrous plan and it has to be repealed and replaced.” – Donald Trump
“Not only are your rates going up by numbers that nobody believes, but your deductibles are going up. So that unless you get hit by a truck, you’re not going to be able to use it. It is a disastrous plan and it has to be repealed and replaced.” – Donald Trump
 Healthcare
Healthcare 



 January 2016 marks the 3rd year of the Health Insurance Marketplaces, a key provision of the Affordable Care Act designed to help millions of Americans buy affordable, quality healthcare. In those three years, enrollment has grown to well over 12 million people. Thus far, 3 million new Americans enrolled in 2016. 35% of those enrolled are 35 years old or younger; an important statistic for the viability of the law. Without enough young enrollees with minimal healthcare usage, the prices for health plans could potentially skyrocket. 85% of those enrolled are receiving financial assistance, which make the costs of their health plans cheaper each month.
January 2016 marks the 3rd year of the Health Insurance Marketplaces, a key provision of the Affordable Care Act designed to help millions of Americans buy affordable, quality healthcare. In those three years, enrollment has grown to well over 12 million people. Thus far, 3 million new Americans enrolled in 2016. 35% of those enrolled are 35 years old or younger; an important statistic for the viability of the law. Without enough young enrollees with minimal healthcare usage, the prices for health plans could potentially skyrocket. 85% of those enrolled are receiving financial assistance, which make the costs of their health plans cheaper each month.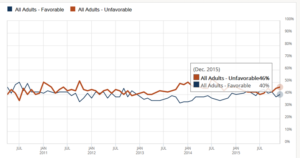
{kind=link}
{kind=link}
{kind=link}